
IVF Centre in Ambala, Haryana
For parenthood, many people opt for In Vitro Fertilization, which is modern reproductive technology (ART) and commonly referred to as IVF. But for positive results, one should choose the best IVF Centre.
Jaspal Hospital is a standalone IVF Centre in Ambala City with an excellent and experienced team of IVF specialists and embryologists, who are able to offer you today’s most advanced and effective procedures in IVF treatment. Our IVF Specialists and embryologists have been trained and have worked in some of the Best IVF Centers in the world. Jaspal Hospital in Ambala City aims to give you the best chance of having a healthy baby, while providing you with a calm environment to make you feel at home. Our team of IVF experts, clinical and support staff is committed to provide you with the best possible care and advice that you can trust.


The Process
Our Services
Jaspal Hospital’s IVF Centre, a well known IVF centre in Ambala City, Haryana offers the complete range of assisted reproduction treatments in an atmosphere of personalized care and empathy towards our patients. Our Infertility center has the best Infertility Specialists in Ambala, and is supported by fully equipped laboratory facilities including genetic testing and counseling. As our patient, you will be guided with complete transparency through selecting options and going through your treatment plan.
FERTILITY ASSISTANCE
- IVF – In Vitro Fertilization
- IUI – Intrauterine Insemination
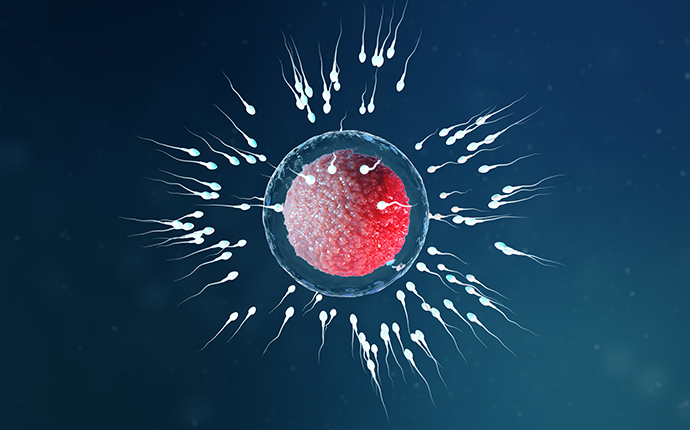
- ICSI – Intracytoplasmic Sperm Injection
- Treating Multiple Prior Failed IVF Cycles
- IVF Pregnancy Care
MALE INFERTILITY
- Surgical Sperm Retrieval
- MESA – Microsurgical Epididymal Sperm Aspiration
- TESA – Testicular Sperm Aspiration
- TESE – Testicular Sperm Extraction
- PESA – Percutaneous Epididymal Sperm Aspiration

Diagnosis
- Semen Analysis
- Hormonal Study
- Pelvic Ultrasound
- Tubal Patency Test
- Follicular Monitoring
- Sperm DNA Fragmentation Test

FREEZING FACILITIESE
- FET – Frozen Embryo Transfer
- Surrogacy
- Donor Eggs
- Donor Sperm
DIAGNOSTIC, OPERATIVE, LAPAROSCOPY AND HYSTEROSCOPY
- PCOS
- Endometriosis
- Fibroids
- Cysts, etc
THIRD PARTY REPRODUCTION
- Donor Eggs
- Sperm Donation
- Embryo Donation
- Surrogacy
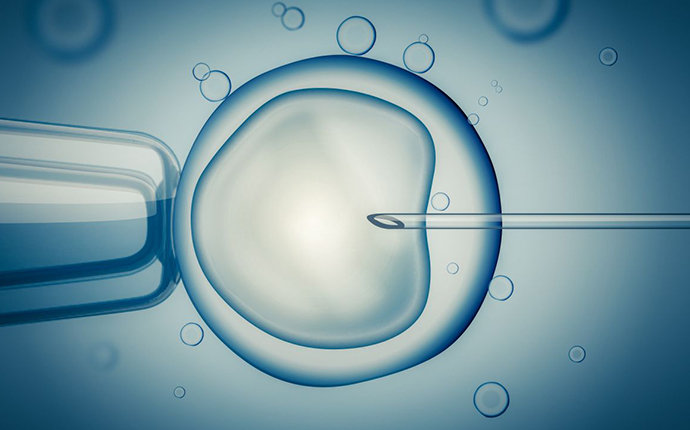
What exactly IVF treatment is?
IVF (In-Vitro Fertilization) is a type of assisted reproductive technology which involves a series of procedures to treat fertility and assist with the conception of child. During IVF, mature eggs are collected (retrieved) from your ovaries and fertilized by sperm in a lab. It is true that both men and women have an equal likelihood of suffering from infertility. Due to increased work stress, hectic and fast-paced urban lifestyle, environmental toxins, and delaying marriageable age – the chances of infertility are rising significantly.
Sometimes, a reason inexplicable to infertility may cause more frustration and depression in couple’s life. Therefore, it is important to opt for a fertility treatment process that assures you. We at Jaspal Hospital are committed to offering the best and ethical treatment for fertility and assisted reproduction.
IVF or In-Vitro Fertilization is a process where the egg is retreived and combined with the sperm outside the body i.e., in-glass fertilization, and the fertilized embryo is then transferred to the uterus.
In some cases where the patient uterus is not favourable for the pregnancy we also provide surrogates for them where the surrogate uterus is used for the pregnancy, and the resulting child born is genetically unrelated to the surrogate.
The cause of infertility may include Hormonal imbalance in both men or women, trouble in ovulation in women, problem with fallopian tubes or uterus and some other undiagnosed reason will be possible.
Infertility treatment at Jaspal Hospital is precise and success oriented. Our state-of-the-art facility and highly experienced doctors provide exceptional treatment options for various infertility conditions.



Frequently Asked Questions
When is IVF Needed?
Because the IVF process bypasses the fallopian tubes (it was originally developed for women with blocked or missing fallopian tubes), it is the procedure of choice for those with fallopian tube issues, as well as for such conditions as endometriosis, male factor infertility and unexplained infertility. A physician can review a patient’s history and help to guide them to the treatment and diagnostic procedures that are most appropriate for them.
Are there risks to having a baby through IVF?
While some research suggests a slightly higher incidence of birth defects in IVF-conceived children compared with the general population (4 – 5% vs. 3%), it is possible that this increase is due to factors other than IVF treatment itself.
It is important to recognize that the rate of birth defects in the general population is about 3% of all births for major malformations and 6% if minor defects are included. Recent studies have suggested that the rate of major birth defects in IVF-conceived children may be on the order of 4 to 5%. This slightly increased rate of defects has also been reported for children born after IUI and for naturally-conceived siblings of IVF children, thus it is possible that the risk factor is inherent in this particular patient population rather than in the technique used to achieve conception.
Research indicates that IVF-conceived children are on par with the general population in academic achievement as well as with regards to behavioral and psychological health. More studies are under way to further investigate this important issue.
Do fertility hormones pose long term health risks?
Compared with the general population, women who have never conceived appear to have a slightly increased risk of ovarian cancer (about 1.6 times the rate). Because it is thought that many of these women have also used fertility medications, it has been hypothesized that a link might exist between fertility medications and this particular cancer. A number of studies have been conducted since 1992 when this concern was first raised. None have found an association between fertility medications and higher risk of ovarian or between IVF treatment itself and higher risk of ovarian cancer. Preliminary results from an ongoing National Institutes of Health study likewise suggest no association between fertility medications and ovarian, uterine or breast cancer.
It is possible that this association is due not to the use of fertility medication, but to the fact that this population of women has never undergone childbirth. Findings from the National Institutes of Health and others suggest that pregnancy or some component of the childbearing process may in fact protect directly against ovarian cancer.
Are IVF injections painful?
The prospect of daily injections can be overwhelming. While injections are a necessary part of IVF treatment, we have designed our medication schedules and injection type to minimize discomfort and stress; and our nurses carefully instruct and support every patient throughout this process. Medications that once had to be injected into the muscle have been replaced by medications given as a small injection under the skin (subcutaneous). Such injections are most commonly taken over a 10-12 day period, followed by one intramuscular injection of hCG, a hormone that triggers ovulation at the conclusion of the stimulation cycle. The hCG injection, previously only available in an intramuscular form, is now available in a subcutaneous form (Ovidrel) for patients that wish to avoid intramuscular injection. Although the recombinant subcutaneous form of hCG in Ovidrel has not been around as long as intramuscular hCG, all indications are that it is just as effective.
After egg retrieval, patients are given a progesterone hormone supplement in order to prepare the lining of the uterus for the embryo transfer. For most patients, progesterone may be taken in a vaginal tablet or vaginal suppository form rather than an injection. In this way, injections may be avoided entirely during the second half of the IVF cycle. Progesterone vaginal tablets and suppositories have been proven to be as effective as progesterone injections.
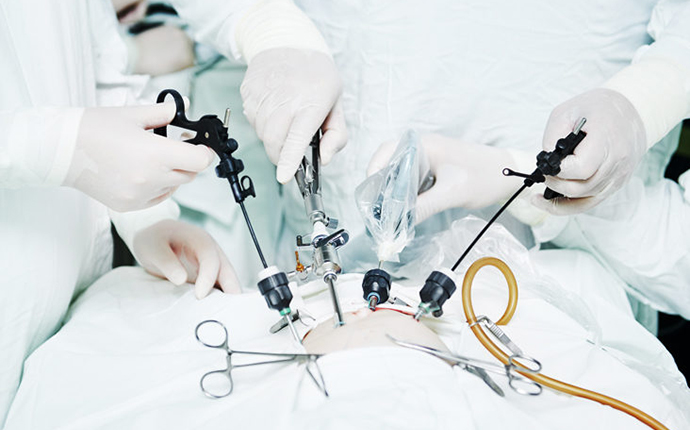
Is the egg retrieval procedure painful?
Because anesthesia is used for egg retrieval, patients feel nothing during the procedure. Egg retrieval is a minor surgery, in which a vaginal ultrasound probe fitted with a long, thin needle is passed through the wall of the vagina and into each ovary. The needle punctures each egg follicle and gently removes the egg through a gentle suction. Anesthesia wears off quickly once egg retrieval is concluded. Patients may feel some minor cramping in the ovaries that can be treated with appropriate medications.
How soon can out of town patients travel home after IVF treatment?
Most of our out of town patients return home the day after the embryo transfer — there is no medical reason to stay in San Francisco after IVF treatment. All types of travel are safe. Sitting for an extended period of time will not affect chances of pregnancy. We recommend that patients traveling by air drink plenty of fluids, as circulated air can be quite dry, and dehydration should be avoided.
Is IVF using up all a woman's eggs?
A woman’s ovaries house hundreds of potential eggs. Each month, during the natural ovulation cycle, the ovary selects just one egg from a pool of 100-1,000. Those eggs which are not selected undergo a natural cell death process called atresia. When a woman uses fertility medication, the body’s natural selection process is overridden, and a number of these otherwise unused eggs are allowed to grow. As many as 20 eggs may be stimulated in a given cycle. Thus when using fertility medication in the IVF process, not only is the woman not using up all of her eggs, but she is ‘rescuing’ eggs that otherwise would have undergone atresia.
What are the chances of pregnancy with frozen embryos?
In general, the success of frozen-thawed embryo transfer procedures depends on three factors:
- The quality and survival of the frozen-thawed embryos. In general, we only freeze good quality embryos so the current rate of survival is greater than 90%.
- The age of the woman who produced the eggs. In patients under the age of 37, the chances of pregnancy with frozen-thawed embryos are similar to a pregnancy with fresh embryos.
- In patients 37 years or older, pregnancy chances with frozen-thawed embryos decline in conjunction with declining fertility in general, but still can be quite good. As always it is best to discuss a woman’s individual situation with their physician.
- The status of the uterus in the woman receiving the embryos. A healthy endometrial lining free of any interfering fibroids or polyps provides a sound environment for embryo implantation.
How are frozen embryos transferred?
Previously frozen embryos may be transferred during a woman’s natural cycle or in a controlled (artificial) cycle, depending on a number of factors:
Controlled cycle transfer.
In a controlled cycle, hormone medications are given to prepare the uterus for transfer. This method is recommended for patients who have irregular cycles. Because the controlled cycle can be precisely timed, it is also advised for those who are on a set travel schedule. The medications commonly used for a controlled cycle are estrogen (either in an injectable or oral form) and progesterone (in either an injectable or vaginal form).
Natural cycle transfer.
Patients who have a regular menstrual cycle may have the option of using their natural cycle for transfer of frozen-thawed embryos. In this case, there is no need for hormone treatment, as the body’s natural cycle will prepare the uterus for pregnancy. In cases where natural cycle transfer is possible, this option allows for less medication and monitoring and thus is often relatively affordable for patients. We typically will monitor the natural cycle using home urinary ovulation predictor kits as well as ultrasounds. When the kit changes and/or a nice pre-ovulatory follicle is seen on ultrasound, we administer a single injection of Ovidrel (recombinant subcutaneous hCG) and the patient starts progesterone vaginal suppositories a couple of days later. The embryo transfer will occur 5-7 days after ovulation/hCG injection, depending on whether the embryos are frozen at a Day 3 or Day 5 stage.
For the transfer procedure itself, the embryo is thawed at room temperature, and then warmed to body temperature (37° C). As with a fresh embryo transfer, embryos are placed inside a special catheter (a very thin tube), which is guided through the cervix and into the uterus. Embryos are gently injected into the uterus and the catheter is removed. This procedure requires no anesthesia, and is done in a position similar to a pelvic examination for a Pap smear. After transfer, the woman rests for 15 minutes and then is able to go home, where a day of rest or very gentle daily activity is recommended.
What are the options if a woman's own eggs are not producing a pregnancy?
The ability to use a donor egg has enabled thousands of women to become pregnant when they otherwise might not have had this opportunity. While a woman’s eggs may not be viable, very often the uterus is completely healthy and capable of supporting a pregnancy. In these cases, egg donation with IVF has high success rates. This procedure follows the same protocol as IVF, except the intended parents select a donor and use the donor’s egg to create the embryo. Patients may seek egg donation services at Jaspal Hospital Egg Donor Agency or at an outside agency.
What if a woman is not capable of carrying a pregnancy?
Various medical conditions may make it impossible for a woman to carry a pregnancy. Reproductive medicine provides the option of enabling another woman, known as a gestational carrier (formerly called a surrogate) to carry the child of a woman who cannot sustain a pregnancy.
There are two types of gestational carriers:
- A traditional gestational carrier becomes artificially inseminated with the sperm of the intended father and uses her own eggs to fertilize the embryo. Many fertility centers, including Pacific Fertility Center do not offer traditional surrogacy. The legal issues and complicated past history of parental rights with traditional surrogacy have led us to discourage this option.
- A gestational carrier with IVF does not contribute any of her own genetic material. In this case, the egg as well as sperm are extracted from the prospective parents, fertilized in the laboratory with IVF and then implanted into the uterus of the surrogate.
A gestational carrier may be appropriate for those in the following situations:
- No uterus
- Abnormal uterine cavity
- Several recurrent miscarriages
- Recurrent IVF cycles have not produced a pregnancy
- Medical conditions would make pregnancy dangerous for the mother or her baby